L’importance de la gestion du volume
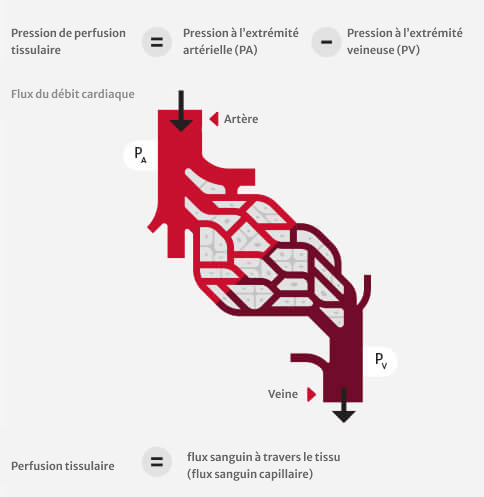
Physiologie de la perfusion : pression et débit
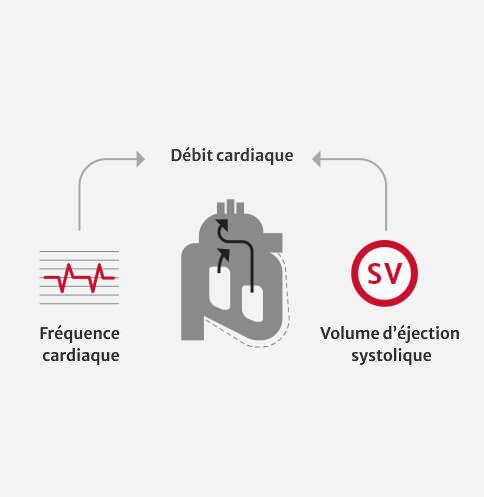
Débit cardiaque (CO) = Volume d’éjection systolique x Fréquence cardiaque
Gestion des paramètres de débit de la perfusion
Il est essentiel de maintenir les patients dans la plage de volume optimale. L’utilisation de paramètres dynamiques et basés sur le débit pour guider l’administration de fluides permet de maintenir les patients dans la plage de volume optimale.1
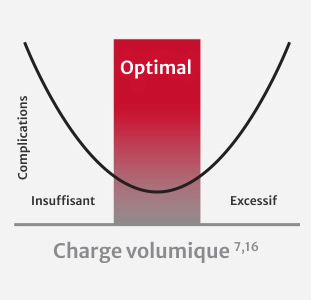
L’administration d’un volume insuffisant est associée à :
- Un dysfonctionnement gastro-intestinal (iléus postopératoire, PONV, hémorragie gastro-intestinale supérieure, fuite anastomotique)2
- Une complication infectieuse (hypoperfusion tissulaire)2,3
- Une défaillance ou une insuffisance rénale aiguë4
L’administration d’un volume excessif est associée à :
- Un œdème pulmonaire5
- Un dysfonctionnement gastro-intestinal (syndrome des loges abdominales, iléus, fuite anastomotique)17,18,19
- Une coagulopathie5
Individualisation de la gestion du volume
Précharge : tension des fibres myocardiques en fin de diastole, résultant du volume du ventricule
Volume d’éjection systolique (SV) : volume de sang pompé par le ventricule gauche à chaque battement de cœur
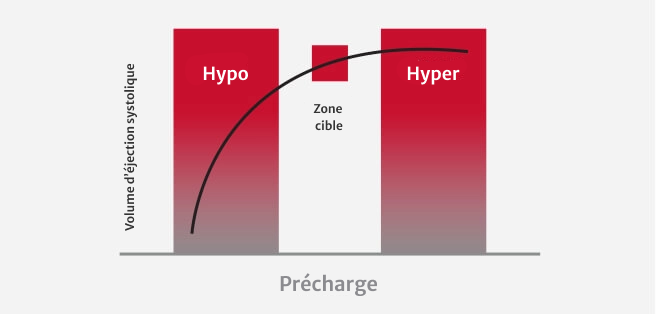
Lors de la gestion de la perfusion, le volume d’éjection systolique peut être optimisé en utilisant la courbe de Frank-Starling du patient, un tracé du volume d’éjection systolique (SV) en fonction de la précharge.
Le volume d’éjection systolique est optimisé lorsqu’il se trouve sur l’épaule de la courbe de Frank-Starling (voir la figure ci-dessous).
L’emplacement du patient sur sa courbe de Frank-Starling peut être déterminé en mesurant le ΔSV en réponse à la modification de la précharge à l’aide de :
Épreuve de remplissage (bolus de fluides)
Lever de jambe passif (PLR)
Les paramètres dynamiques, basés sur le débit, sont plus instructifs que les paramètres conventionnels pour déterminer la réactivité aux fluides et peuvent aider à éviter une administration de fluides excessive ou insuffisante.7
Des études cliniques ont montré que les méthodes classiques de gestion du volume, basées sur des paramètres conventionnels, sont erronées et peu sensibles.6
Les paramètres hémodynamiques avancés, comme le volume d’éjection systolique (SV) et la variation du volume d’éjection systolique (SVV), sont essentiels à l’administration optimale de fluides.6
La SVV s’est avérée être un indicateur très sensible et spécifique de la réactivité de la précharge dans la gestion de la perfusion. En tant que paramètre dynamique, la SVV s’est avérée être un facteur prédictif précis de la réactivité des fluides dans les conditions de charge induites par la ventilation mécanique.6,8,20
Recherche démontrant la valeur des paramètres dynamiques et basés sur le débit
- Thacker, et al. Perioperative Fluid Utilization Variability and Association With Outcomes: Considerations for Enhanced Recovery Efforts in Sample US Surgical Population.Ann Surg 2015
- Peng, K., et al., Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery.Med Princ Pract, 2014
- Dalfino et al. Haemodynamic goal-directed therapy and postoperative infections: earlier is better. A systematic review and meta-analysis.Crit Care 2011
- Giglio, MT et al. Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery: a meta-analysis of randomized controlled trials.British Journal of Anesthesia 2009
- Shin, C. et al. Effects of Intraoperative Fluid Management on Postoperative Outcomes: A Hospital Registry Study.Annals of Surgery 2017
- Sun, Y. et al. Effect of perioperative goal-directed hemodynamic therapy on postoperative recovery following major abdominal surgery-a systematic review and meta-analysis of randomized controlled trials.Critical Care 2017
- Goepfert, M.S., et al., Individually optimized hemodynamic therapy reduces complications and length of stay in the intensive care unit: a prospective, randomized controlled trial.Anesthesiology, 2013
Pour en savoir plus sur la gestion des fluides avec des paramètres avancés, communiquez avec nous dès aujourd’hui.
Réduction de la variabilité grâce au traitement péri-opératoire orienté vers les objectifs (PGDT)
Les complications post-chirurgicales ont un impact sur l’homme.9

Des complications majeures surviennent dans environ 16 % des interventions chirurgicales.9

Indépendamment du risque préopératoire pour le patient, la survenue d’une seule complication post-chirurgicale dans les 30 jours réduit la survie médiane des patients de 69 %.10

Il a été démontré que l’optimisation hémodynamique par le PGDT permet de réduire les complications comme l’insuffisance rénale aiguë (AKI) et l’infection du site chirurgical (SSI), mais la durée d’hospitalisation et les coûts associés chez les patients opérés présentant un risque modéré à élevé.11,12
L’optimisation hémodynamique par le PGDT peut :
Réduire les complications post-chirurgicales de 32 % en moyenne13

Réduire la durée moyenne de l’hospitalisation d’un jour ou plus13,14

Coût supplémentaire approximatif du traitement d’une complication post-opératoire : 18 000 à 20 000 $15
Le PGDT est un protocole de traitement utilisant des paramètres hémodynamiques dynamiques et basés sur le débit dans le but de prendre les décisions appropriées en matière de gestion du volume. Le PGDT peut être mis en œuvre dans le cadre d’une procédure unique ou d’une initiative plus vaste, comme les parcours de récupération améliorée après une intervention chirurgicale.
Plus de 50 études démontrant l’utilisation du PGDT
Plus de 50 essais contrôlés aléatoires et plus de 14 méta-analyses ont démontré l’intérêt clinique de l’optimisation hémodynamique par rapport à la gestion standard du volume.
Études
- Michard, et al. Perioperative goal-directed therapy with uncalibrated pulse contour methods: impact on fluid management and postoperative outcome.British Journal of Anesthesia 2017
- Pearse, R. et al. Effect of a Perioperative, Cardiac Output–Guided Hemodynamic Therapy Algorithm on Outcomes Following Major Gastrointestinal Surgery A Randomized Clinical Trial and Systematic Review.JAMA 2014
- Grocott, MP et al. Perioperative increase in global blood flow to explicit defined goals and outcomes after surgery: a Cochrane Systematic Review.British Journal of Anesthesia 2013
- Thiele et al. American Society for Enhanced Recovery (ASER) and Perioperative Quality Initiative (POQI) joint consensus statement on perioperative fluid management within an enhanced recovery pathway for colorectal surgery.Periop Med 2016
- Ramsingh et al. Outcome impact of goal directed fluid therapy during high risk abdominal surgery in low to moderate risk patients: a randomized controlled trial.J Clin Monit Comput 2011
- Cecconi, et al. Goal directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia.Crit Care 2011
Voir la liste complète des études
Essais contrôlés aléatoires montrant un avantage du traitement péri-opératoire orienté vers les objectifs
Plus de 3 000 patients ont été recrutés dans ces 52 RCT positifs.

| Titre, auteur et année | n | Paramètres optimisés | Chirurgie | Outil | Principaux avantages |
| Prospective trial of supranormal values of survivors as therapeutic goals in high-risk patients. Shoemaker, 1988 | 310 | DO2 | Générale | PAC-1 | Morbidité Mortalité (21 contre 34 %) Économies de coûts |
| Preoperative optimization of cardiovascular hemodynamics improves outcomes in peripheral vascular surgery. Berlauk,1991 | 89 | CI, PCWP, SVR | Vasculaire | PAC-2 | Morbidité |
| Prospective trial of supranormal values as goals of resuscitation in severe trauma. Fleming, 1992 | 67 | DO2 | Traumatisme | PAC-3 | Morbidité |
| A randomized clinical trial of the effect of deliberate perioperative increase of oxygen delivery on mortality in high-risk patients. Boyd, 1993 | 107 | DO2 | Générale | PAC-4 | Morbidité Mortalité (6 contre 22 %) Économies de coûts |
| Perioperative plasma volume expansion reduces the incidence of gut mucosal hypoperfusion during cardiac surgery. Mythen, 1995 | 60 | SV | Cardiaque | Doppler-1 | Morbidité Durée d’hospitalisation |
| Intraoperative intravascular volume optimisation and length of hospital stay after repair of proximal femoral fracture: randomised controlled trial. Sinclair, 1997 | 40 | SV | Hanche | Doppler-2 | Durée d’hospitalisation |
| Response of patients with cirrhosis who have undergone partial hepatectomy to treatment aimed at achieving supranormal oxygen delivery and consumption. Ueno, 1998 | 34 | DO2 | Hépatectomie | PAC-5 | Morbidité |
| Reducing the risk of major elective surgery: randomised controlled trial of preoperative optimization of oxygen delivery. Wilson, 1999 | 138 | DO2 | Générale et vasculaire | PAC-6 | Morbidité Durée d’hospitalisation Économies de coûts |
| A prospective, randomized study of goal-oriented hemodynamic therapy in cardiac surgical patients. Polonen, 2000 | 393 | SvO2 | Cardiaque | PAC-7 | Morbidité Durée d’hospitalisation |
| Effects of maximizing oxygen delivery on morbidity and mortality in high-risk surgical patients. Lobo, 2000 | 37 | DO2 | Générale | PAC-8 | Morbidité Mortalité (16 contre 50 %) |
| Randomized controlled trial to investigate influence of the fluid challenge on duration of hospital stay and perioperative morbidity in patients with hip fractures. Venn, 2002 | 59 | SV | Hanche | Doppler-3 | Morbidité |
| Goal-directed Intraoperative fluid administration reduces length of hospital stay after major surgery. Gan, 2002 | 100 | SV | Générale | Doppler-4 | Morbidité Durée d’hospitalisation |
| Randomised controlled trial investigating the influence of intravenous fluid titration using oesophageal Doppler monitoring during bowel surgery. Conway, 2002 | 57 | SV | Intestinale | Doppler-5 | Morbidité |
| Randomised controlled trial assessing the impact of a nurse delivered, flow monitored protocol for optimisation of circulatory status after cardiac surgery. McKendry, 2004 | 174 | SV | Cardiaque | Doppler-6 | Durée d’hospitalisation |
| Intraoperative oesophageal Doppler guided fluid management shortens postoperative hospital stay after major bowel surgery. Wakeling, 2005 | 128 | SV | Intestinale | Doppler-7 | Morbidité Durée d’hospitalisation |
| Early goal-directed therapy after major surgery reduces complications and duration of hospital stay. A randomised, controlled trial. Pearse, 2005 | 122 | DO2 | Générale | LidCO-1 | Morbidité Durée d’hospitalisation |
| Randomized clinical trial assessing the effect of Doppler- optimized fluid management on outcome after elective colorectal resection. Noblett, 2006 | 108 | SV | Intestinale | Doppler-8 | Morbidité Durée d’hospitalisation |
| Esophageal Doppler-guided fluid management decreases blood lactate levels in multiple-trauma patients: a randomized controlled trial. Chytra, 2007 | 162 | SV | Traumatisme | Doppler-9 | Morbidité Durée d’hospitalisation |
| Goal-directed fluid management based on pulse pressure variation monitoring during high-risk surgery: a pilot randomized controlled trial. Lopes, 2007 | 33 | PPV | Générale | Ligne A-1 | Morbidité Durée d’hospitalisation |
| Goal-directed intraoperative therapy reduces morbidity and length of hospital stay in high-risk surgical patients. Donati, 2007 | 135 | ERO2 | Générale et vasculaire | CVC-1 | Morbidité Durée d’hospitalisation |
| Goal-directed intraoperative therapy based on Autocalibrated arterial pressure waveform analysis reduces hospital stay in high-risk surgical patients: a randomized, controlled trial. Mayer, 2009 | 60 | SVV, SVI, CI | Abdominale | Capteur FloTrac-1 | Morbidité Durée d’hospitalisation |
| Intraoperative fluid optimization using stroke volume variation in high risk surgical patients: results of prospective randomized study. Benes, 2010 | 120 | SVV, CI | Abdominale et vasculaire | Capteur FloTrac-2 | Morbidité |
| Haemodynamic optimisation improves tissue microvascular flow and oxygenation after major surgery: a randomised controlled trial. Jhanji, 2010 | 135 | SV, DO2 | Abdominale | LidCO-2 | Morbidité |
| Goal-directed haemodynamic therapy during elective total hip arthroplasty under regional anaesthesia. Cecconi, 2011 | 40 | DO2 | Hanche | Capteur FloTrac-3 | Morbidité |
| A double-blind randomized controlled clinical trial to assess the effect of doppler optimized intraoperative fluid management on outcome following radical cystectomy. Pillai, 2011 | 66 | SV | Cystectomie | Doppler-10 | Morbidité |
| Haemodynamic optimisation in lower limb arterial surgery: room for improvement? Bisgaard, 2012 | 40 | SV, DO2 | Vasculaire | LidCO-3 | Morbidité |
| Outcome impact of goal directed fluid therapy during high risk abdominal surgery in low to moderate risk patients: a randomized controlled trial. Ramsingh, 2012 | 38 | SVV | Abdominale | Capteur FloTrac-4 | Morbidité Durée d’hospitalisation |
| Goal-directed intraoperative fluid therapy guided by stroke volume and its variation in high-risk surgical patients: a prospective randomized multicentre study. Scheeren, 2012 | 40 | SVV, SV | Abdominale | Capteur FloTrac-5 | Morbidité |
| Intraoperative fluid management in open gastrointestinal surgery: goal-directed versus restrictive. Zhang, 2013 | 80 | SVV, CI | Thoracique | Capteur FloTrac-6 | Morbidité |
| Individually optimized hemodynamic therapy reduces complications and length of stay in the Intensive Care Unit. Goepfert, 2013 | 100 | SVV, GEDI, CI, EVLW | Cardiaque | PiCCO-1 | Morbidité |
| Perioperative goal-directed hemodynamic therapy based on radial arterial pulse pressure variation and continuous cardiac index trending reduces postoperative complications after major abdominal surgery: a multi-center, prospective, randomized study. Salzwedel, 2013 | 160 | PPV, CI | Abdominale | ProAQT-1 | Morbidité Durée d’hospitalisation |
| Goal-directed fluid therapy in gastrointestinal surgery in older coronary heart disease patients: randomized trial. Zheng, 2013 | 60 | SVV, SVI, CI | Abdominale | Capteur FloTrac-7 | Morbidité Durée d’hospitalisation |
| Zakhaleva, J., et al., The impact of intravenous fluid administration on complication rates in bowel surgery within an enhanced recovery protocol: a randomized controlled trial. Colorectal Dis, 2013. 15(7): p. 892-9 | 91 | SV | Chirurgie abdominale | TED | Morbidité |
| Peng, K., et al., Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery. Med Princ Pract, 2014. 23(5): p. 413-20 | 80 | SVV | Chirurgie orthopédique | Capteur PC FloTrac | Rétablissement gastro-intestinal |
| Zeng, K., et al., The influence of goal-directed fluid therapy on the prognosis of elderly patients with hypertension and gastric cancer surgery. Drug Des Devel Ther, 2014. 8: p. 2113-9 | 60 | SVV | Gastrectomie | Capteur PC FloTrac | Morbidité, durée d’hospitalisation |
| Colantonio, L., et al., A randomized trial of goal directed vs. standard fluid therapy in cytoreductive surgery with hyperthermic intraperitoneal chemotherapy. J Gastrointest Surg, 2015. 19(4): p. 722-9 | 80 | CI, SVI | Chirurgie cytoréductrice | Capteur PC FloTrac | Morbidité, durée d’hospitalisation |
| Funk, D.J., et al., A randomized controlled trial on the effects of goal-directed therapy on the inflammatory response open abdominal aortic aneurysm repair. Crit Care, 2015. 19: p. 247 | 40 | SVV, CI | Chirurgie vasculaire | Capteur PC FloTrac | Morbidité |
| Mikor, A., et al., Continuous central venous oxygen saturation assisted intraoperative hemodynamic management during major abdominal surgery: a randomized, controlled trial. BMC Anesthesiol, 2015. 15: p. 82 | 79 | ScvO2 | Chirurgie abdominale | CVC Cevox | Mortalité et apport d’oxygène |
| Han, G., et al., Application of LiDCO-Rapid in peri-operative fluid therapy for aged patients undergoing total hip replacement. International Journal of Clinical and Experimental Medicine, 2016. 9(2): p. 4473-4478 | 40 | SVV | Chirurgie orthopédique | PC LiDCO rapide | Morbidité |
| Hand, W.R., et al., Intraoperative goal-directed hemodynamic management in free tissue transfer for head and neck cancer. Head Neck, 2016. 38 Suppl 1: p. E1974-80 | 94 | SVV, CI, SVR | Chirurgie des tissus libres | Capteur PC FloTrac | Durée du séjour en USI |
| Kapoor, P.M., et al., Perioperative utility of goal-directed therapy in high-risk cardiac patients undergoing coronary artery bypass grafting: “A clinical outcome and biomarker- based study”. Ann Card Anaesth, 2016. 19(4): p. 638-682 | 130 | SVV, CI, SVI, SVRI, DO2 | Chirurgie cardiaque | Capteur PC FloTrac, CVC d’oxymétrie Edwards | Durée du séjour en USI, durée d’hospitalisation |
| Kumar, L., S. Rajan et R. Baalachandran, Outcomes associated with stroke volume variation versus central venous pressure guided fluid replacements during major abdominal surgery. J Anaesthesiol Clin Pharmacol, 2016. 32(2): p. 182-6 | 60 | SVV | Chirurgie abdominale | Capteur PC FloTrac | Durée du séjour en USI |
| Osawa, E.A., et al., Effect of Perioperative Goal-Directed Hemodynamic Resuscitation Therapy on Outcomes Following Cardiac Surgery: A Randomized Clinical Trial and Systematic Review. Crit Care Med, 2016. 44(4): p. 724-33 | 126 | CI, SVI | Chirurgie cardiaque | PC LiDCO rapide | Morbidité, durée du séjour en USI, durée d’hospitalisation |
| Yuanbo, Z., et al., ICU management based on PiCCO parameters reduces duration of mechanical ventilation and ICU length of stay in patients with severe thoracic trauma and acute respiratory distress syndrome. Annals of Intensive Care, 2016. 6(1): p. 113 | 264 | ITBVI, EVLWI, CI | Traitement du SDRA en USI | PC PiCCO | Jours de ventilation mécanique, durée du séjour en USI et économies de coûts |
| Elgendy, M.A., I.M. Esmat et D.Y. Kassim, Outcome of intraoperative goal-directed therapy using Vigileo/FloTrac in high-risk patients scheduled for major abdominal surgeries: A prospective randomized trial. Egyptian Journal of Anaesthesia, 2017 | 86 | SVV, CI, MAP | Chirurgie abdominale majeure | Capteur PC FloTrac | Morbidité, durée du séjour en USI |
| Kapoor, P.M., et al., Goal-directed therapy improves the outcome of high-risk cardiac patients undergoing off-pump coronary artery bypass. Ann Card Anaesth, 2017. 20(1): p. 83-89 | 163 | SVV, CI, ScvO2 | Chirurgie cardiaque | Ensemble VolumeView, capteur PC FloTrac | Durée du séjour en USI, durée d’hospitalisation |
| Kaufmann, K.B., et al., Oesophageal Doppler guided goal-directed haemodynamic therapy in thoracic surgery - a single centre randomized parallel-arm trial. Br J Anaesth, 2017. 118(6): p. 852-861 | 100 | SV, CI MAP | Chirurgie thoracique | TED | Morbidité, durée d’hospitalisation |
| Liang, M., et al., Effect of goal-directed fluid therapy on the prognosis of elderly patients with hypertension receiving plasmakinetic energy transurethral resection of prostate. Int J Clin Exp Med, 2017. 10(1): p. 1290-1296 | 60 | SVV | Urologique : résection de la prostate | Capteur PC FloTrac | Morbidité, durée d’hospitalisation |
| Luo, J., et al., Goal-directed fluid restriction during brain surgery: a prospective randomized controlled trial. Ann Intensive Care, 2017. 7(1): p. 16 | 145 | SVV, CI | Neuro-chirurgie | Capteur PC FloTrac | Durée du séjour en USI, économies de coûts, morbidité |
| Weinberg, L., et al., Restrictive intraoperative fluid optimisation algorithm improves outcomes in patients undergoing pancreaticoduodenectomy: A prospective multicentre randomized controlled trial. PLoS One, 2017. 12(9): p. e0183313 | 52 | SVV, CI | Abdominale | Capteur PC FloTrac | Morbidité, durée d’hospitalisation |
| Wu, C.Y., et al., Comparison of two stroke volume variation-based goal-directed fluid therapies for supratentorial brain tumour resection: a randomized controlled trial. Br J Anaesth, 2017. 119(5): p. 934-942 | 80 | SVV | Neuro-chirurgie | Capteur PC FloTrac | Durée du séjour en USI, morbidité |
| Wu, J., et al., Goal-directed fluid management based on the auto-calibrated arterial pressure-derived stroke volume variation in patients undergoing supratentorial neoplasms surgery. INTERNATIONAL JOURNAL OF CLINICAL AND EXPERIMENTAL MEDICINE, 2017. 10(2): p. 3106-3114 | 66 | SVV, CI, MAP | Chirurgie cérébrale | Capteur PC FloTrac | Morbidité, niveaux de lactate |
Références
- Benes, J., Giglio M., Michard, F. (2014) The effects of goal-directed fluid therapy based on dynamic parameters on post-surgical outcome: a meta-analysis of randomized controlled trials. Critical Care, 18(5), 584
- Giglio, MT et al. (2009) Goal-directed haemodynamic therapy and gastrointestinal complications in major surgery: a meta-analysis of randomized controlled trials. British Journal of Anaesthesia, 103(5), 637-46
- Johnson, A., Ahrens, T. (2015) Stroke Volume Optimization: The New Hemodynamic Algorithm. Critical Care Nurse, 35(1), 11-27
- O’Leary, M. (2001) Preventing renal failure in the critically ill. BMJ, 322(7300), 1437-1439
- Holte, K. (2010) Pathophysiology and clinical implications of perioperative fluid management in elective surgery. Danish Medical Bulletin, 57(7), B4156
- Berkenstadt, H., et al. (2001) Stroke Volume Variation as a Predictor of Fluid Responsiveness in Patients Undergoing Brain Surgery. Anesthesia & Analgesia, 92, 984-9
- Cannesson, M. (2010) Arterial pressure variation and goal-directed fluid therapy. Journal of Cardiothoracic and Vascular Anesthesia, 24(3), 487-97
- Peng, K., Li, J., Cheng, H., Ji, FH. (2014) Goal-directed fluid therapy based on stroke volume variations improves fluid management and gastrointestinal perfusion in patients undergoing major orthopedic surgery. Medical Principles and Practice, 23(5), 413-20
- Ghaferi, A., Birkmeyer, J., Dimick, J. (2009) Variation in hospital mortality associated with inpatient surgery. New England Journal of Medicine, 361(14), 1368-75
- Khuri, S., Henderson, W., DePalma, R., Mosca, C., Healey, N., Kumbhani, D. (2005) Determinants of long-term survival after major surgery and the adverse effect of postoperative complications. Annals of Surgery, 242(3), 326-41
- Aya, H., Cecconi, M., Hamilton, M., Rhodes, A. (2013) Goal-directed therapy in cardiac surgery: a systematic review and meta-analysis. British Journal of Anaesthesia, 110(4), 510-7
- Brienza, N., Giglio, M., Marucci, M., Fiore, T. (2009) Does perioperative hemodynamic optimization protect renal function in surgical patients? A meta-analytic study. Critical Care Medicine, 37(6), 2079-90
- Grocott, M., Dushianthan, A., Hamilton, M., Mythen, M., Harrison, D., Rowan, K. (2012) Perioperative increase in global blood flow to explicit defined goals and outcomes following surgery. Cochrane Database of Systematic Reviews, 11, CD004082
- Corcoran, T., Rhodes, J., Clarke, S., Myles, P., Ho, K. (2012) Perioperative fluid management strategies in major surgery: a stratified meta-analysis. Anesthesia & Analgesia, 114(3), 640-51
- Boltz, M., Hollenbeak, C., Ortenzi, G., Dillon, P. (2012) Synergistic implications of multiple postoperative outcomes. American Journal of Medical Quality, 27(5), 383-90
- Bellamy, M. (2006) Wet, dry or something else? British Journal of Anaesthesia, 97(6), 755-7
- Ping W, et al. Effects of Stroke Volume Variability-Guided Intraoperative Fluid Restriction on Gastrointestinal Functional Recovery. Chinese Journal of Anesthesiology 31.1 (2011): 78-81.
- Thacker JKM, et al. Perioperative Fluid Utilization Variability and Association With Outcomes. Annals of Surgery 263.3 (2016): 502-510.
- Durairaj L and Schmidt GA. Fluid Therapy in Resuscitated Sepsis*. Less is More. Recent Advances in Chest Medicine. 133.1 (2008): 252-263.
- Li, Cheng, et al. Stroke Volume Variation for Prediction of Fluid Responsiveness in Patients Undergoing Gastrointestinal Surgery. International Journal of Medical Sciences. 2013; 10(2): 148-155.