IOH is common
88% of patients continuously monitored with an arterial line still experienced hypotension, defined as mean arterial pressure (MAP) <65 for 1 minute.4
Every moment matters

Though intraoperative hypotension (IOH) is common in surgical patients, numerous studies indicate that it is strongly associated with risk of myocardial Injury (MI), acute kidney Injury (AKI), and mortality.1,2 The risks associated with IOH increase with the severity of hypotension.3
88% of patients continuously monitored with an arterial line still experienced hypotension, defined as mean arterial pressure (MAP) <65 for 1 minute.4

Research suggests strong associations between IOH and increased risk of MI, AKI, and mortality in noncardiac surgical patients.1,2,5,6
Acumen Hypotension Prediction Index (HPI) software has been shown to be effective in detecting hemodynamic instability and substantially reducing the amount of intraoperative hypotension during noncardiac surgery, with or without a protocol in patients who received an arterial line.7-11
IOH is a frequent side effect of general anesthesia and is presumed to have unfavorable outcomes for the patient.12 In a multi-center study of over 22,000 noncardiac surgery cases, where all patients received continuous monitoring through an arterial line, 88% of patients had at least one hypotensive event with a mean cumulative duration of 28.2 minutes.4
In a study of 11 hospitals across the U.S., at least one hypotensive event occurred in 88% of noncardiac surgical cases (defined as MAP <65 mmHg for at least 1 min.).4

28.2 minutes (SD 42.6 min) was the mean cumulative duration of hypotension in noncardiac surgery cases (n = 19,446) which had at least 1 minute of hypotension, defined as a MAP <65 mmHg.4

MINS is one of the most common causes of death within 30 days of surgery.1 At least 8 million patients worldwide suffer from MINS each year.13 Research is pointing to a strong association between IOH and increased risk of myocardial and kidney injury in noncardiac surgical patients.5

AKI is a major public health concern linked to poor outcomes, both in terms of health and the patient experience.14 In a recent study of 22,000 noncardiac surgical patients, 11.75% suffered AKI. Several studies also indicate AKI is costly and is associated with incremental increases in length of stay.14-16
A systematic review of the association between IOH and postoperative outcomes conducted by Wesselink et al. indicated that prolonged durations of exposure to lower MAPs were associated with increased risks of end-organ injury comprising of a composite of outcomes including MI, AKI, delirium, stroke, and mortality.12

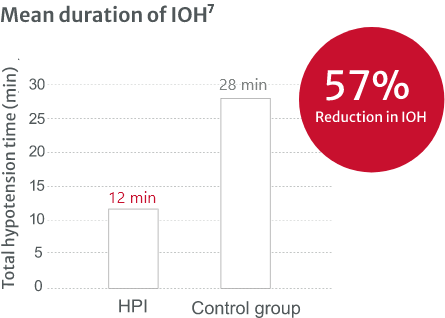
Acumen Hypotension Prediction Index (HPI) software was recently studied in a single arm, multicenter, prospective-to-historical control study at 11 sites where patients received arterial monitoring during noncardiac surgery. In this study, Acumen HPI software has been demonstrated to reduce the duration of IOH by 57%7 for patients who had a hypotensive event.†
These results demonstrate a substantial reduction in mean IOH that was consistent across most sites. Most sites had a >25% reduction in mean duration of IOH, with all sites but one exceeding 35%, (with the results ranging from 23% to 72% mean IOH reduction).7

Acumen HPI software is effective in detecting hemodynamic instability and substantially reducing the amount of IOH.7 It’s the first-of-its-kind predictive decision support software that provides information regarding the likelihood of a patient trending toward hypotension. Acumen HPI software can be unlocked with the noninvasive Acumen IQ cuff‡ or minimally-invasive Acumen IQ sensor.
†A hypotensive event is defined as MAP <65 mmHg for a duration of at least one minute.
‡Surgical patient use only
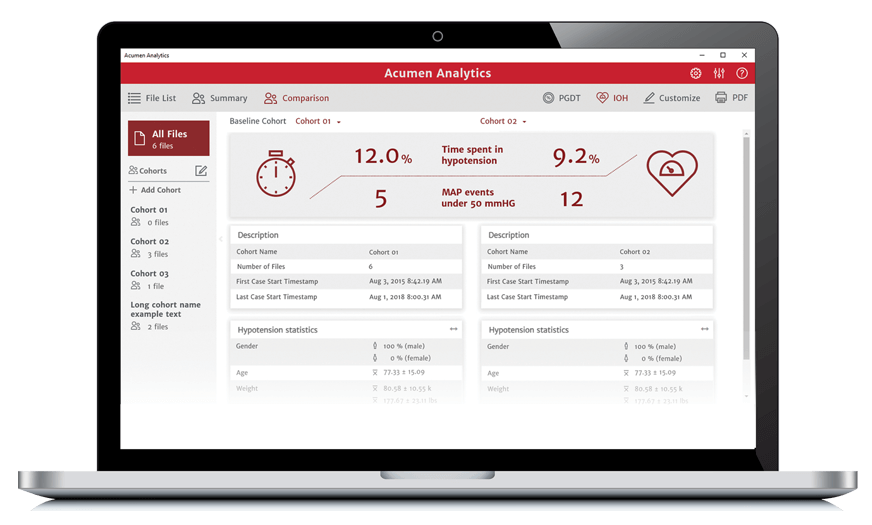
Acumen Analytics software enables you to retrospectively view and analyze hemodynamic parameters including mean arterial pressure, providing you insights into the frequency, duration, and prevalence of intraoperative hypotension in your practice.
With a long-term commitment to improving the quality of care for surgical and critical care patients through education, Edwards clinical education meets you no matter where you are in the learning process — with a continuum of resources and tools that continuously support you as you solve the clinical challenges facing you today, and in the future.
We are committed to providing your institution, clinicians and staff with the highest levels of customer service and support to ensure seamless product implementation and ongoing use, including:
24/7 Technical support
For product information and orders